As we head toward the mid-term elections, affordability has seized center stage in the health care debate, and for good reason. Americans of every class and health status are upset about the amount of money they must shell out to buy insurance and pay the extra bills that arrive after they get sick.
The ruling Republican regime is making things worse. Not only has it launched a full-scale attack on Medicaid, which covers nearly a third of all Americans, the latest White House initiative allows the insurance industry to sell low-cost plans on the Affordable Care Act exchanges that will pay only a fraction of the bills people receive after being hospitalized. If the regime gets its way, comprehensive insurance — the previous requirement for all Obamacare plans — will become unaffordable for almost everyone but the well-to-do.
Democratic Party-oriented think tanks and commentators continue to crank out proposals for making insurance more affordable. A new report from the Searchlight Institute, first reported by Jon Cohn of The Bulwark, calls for limiting private equity’s role in health care; limiting insurers’ ability to abuse prior authorization or hide profits at their wholly-owned physician practices; and wielding antitrust law to bust up hospital and pharmacy benefit manager monopolies.
Last week, Nobel laureate and substacker Paul Krugman laid out his path forward for dealing with the affordability crisis. His three-part explainer started by laying out “why universal healthcare is a desirable objective, and why some type of government intervention is essential to achieve it.”
His second installment described the ongoing Republican assault on Obamacare and its successes. But his final piece, rather than offering a bold or unique plan, or even something like the European countries to which he unfavorably compared the U.S., repeats most Democrats’ long-standing plea for including a public option on the exchanges.
A public option would allow people to buy into Medicare. Progressive groups have been advocating this for decades. The House-backed version of the Affordable Care Act in 2009 included a public option. He imagines many employers would encourage their employees to avail themselves of this new option (presumably providing them with some or most of the cost of the buy-in). “If they like what they get, which they probably would, we could transition over time to a single-payer system without forcing Americans into it,” he wrote.
Shortcomings
Krugman fails to address the virulent opposition that would be mounted against the public option by the hospital, insurance, drug and medical device industries, and the many other types of providers (nursing homes, hospice, ambulatory surgical centers, etc.) that make up the medical industrial complex. Nor does he take into account the main reason employers resist jettisoning their role: It keeps many employees from job-hopping.
Krugman assumes public anger over rising costs will overwhelm their opposition, a dubious proposition in my view even if the Democratic Party wins control over both houses of Congress and the White House. Why do I say dubious?
It is well known that health care accounts for 18 percent of gross domestic product, far more than other industrialized countries. What is less well known is the fact that direct health care provision accounts for 12 percent of all employment in the U.S. It is the largest or second largest employer in almost every city and town. In at least one recent month, the nation would have shed jobs had it not been for growth in the health care sector.
If you throw in employment in the health insurance industry, manufacturers of drugs, medical devices and durable medical equipment, and the small army of consultants, medical educators, think tankers and other health care hangers-on, about one in six American jobs flows from our bloated health care sector. Moreover, they are evenly distributed throughout the country, constituting a powerful voice in every Congressional district.
Reformers need a way to win providers — not the hospital system administrators, not the insurance company executives, not the nursing home operators; but the physicians, nurses and nurse aides, support staff, and more — to their side.
That’s why I am committed to a strategy that provides the health care sector with an off-ramp from its unproductive and wasteful ways. The system is tremendously successful at generating new technologies and treating highly complex cases. But it stinks at almost everything else that the general population needs.
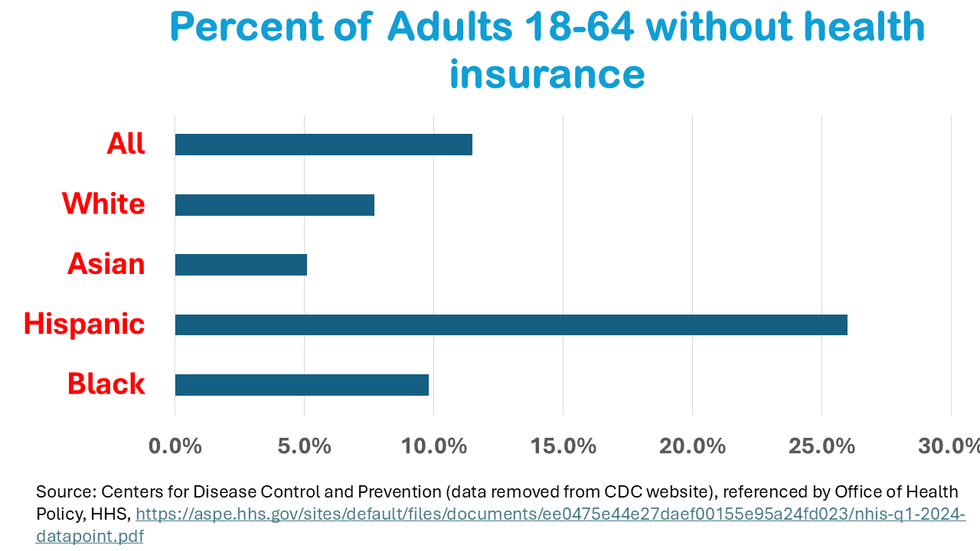
It consumes more societal resources than any country on earth. It doesn’t cover everyone. Its multi-payer complexity requires enormous administrative overhead. Its specialty-driven, fee-for-service payment system delivers more pricey tests and operations than people need. It shortchanges primary care and prevention. It generates worse outcomes than other countries whether measured by longevity, infant and maternal mortality or chronic disease levels. And those lousy outcomes are extremely unfair, with minority populations suffering far worse outcomes than their white fellow Americans. (I will address this issue in my next article.)
I agree with Krugman that the Obamacare exchanges need a public option for the uninsured and for any employer that wants to join. But the details, which he doesn’t address in his article, matter. Its pricing will have to be set at a percentage somewhat larger than what Medicare pays, which is what Washington state did when it became the first state to roll out a public option in 2021 (at 160 percent of Medicare prices). Colorado and Nevada have followed suit with their own higher-than-Medicare priced public options.
Providers need a guaranteed off-ramp. They and their millions of employees can’t absorb the sudden shock to the system required by the mass migration to the public option at Medicare rates, which, according to the Medicare Payment Advisory Commission, are somewhat below breakeven rates. Therefore, in addition to creating the public option, providers need to be regulated through government-set budgets that are set at current levels and guaranteed to grow, but only at a slower rate than the rest of the economy.
Over the past several decades, health care spending has risen faster than the rate of economic growth, ballooning from 13 percent of GDP at the start of this century to 18 percent of GDP today. If budgets are allowed to grow at one to one-and-a-half percentage points above inflation (that’s about half the economic growth rate), U.S. health care spending will gradually decline to international norms.
Invest in health
What else would guaranteed budgets accomplish? It would free hospitals, physician practices, clinics and other provider organizations from the treadmill of fee-for-service medicine, where the more you do the more you make. It would free up resources to invest in the nation’s woefully underfunded primary care and behavioral health providers.
It would encourage provider organizations to invest in community outreach to underserved populations suffering from undiagnosed and untreated diseases (think hypertension, pre-diabetes, obesity, and drug, alcohol and tobacco addiction). If we treat disease before its complications set in, people will spend less time in the emergency room, where care is costliest, and often comes too late to affect the trajectory of their chronic condition.
In short, the nation’s health care system needs to transform itself into one that promotes health, not one that profits when more people get sick. The Make American Healthy Again movement has that part right. Reformers on the left should grab that page from their playbook by providing a positive vision for how to produce healthier individuals as well as a plan to reduce how much the public has to spend.
- Republicans Push Skimpy, Unaffordable Health Coverage As Costs Keep Rising ›
- RFK Jr. Campaign Director Reveals Her True Allegiance Is To Trump ›
- With System's Looming Implosion, Health Care Could Dominate 2026 Elections ›
- Stop The Gouging: A Bold Plan To Make American Health Care Truly 'Affordable' ›
- Erupting Crisis Of Uninsurance, Created By Republicans, Will Soon Engulf US Families - National Memo ›